



Vaccine Mandates for University and College Students
The Latest Stage of Anti-Science COVID Reaction

Our Moment in History
It is perhaps a forgivable conceit that we tend to regard events in our own day as looming larger in the full sweep of history than a proper historical perspective would permit. These are, after all, the only times we’ve ever lived through. Nevertheless, it seems evident to the current generation that the COVID-19 pandemic has assumed a prominent place among the most devastating plagues of human history. The terrible greatness of COVID-19, however, is not in the strength of the virus that brought the pandemic, but in the unprecedented spectacle of a planet-wide reaction to it which has done more harm than the worst plagues of history. The number killed by the COVID lockdowns does not rival the toll taken by the Black Death of the fourteenth century, which killed 30% of the population of Europe. But the pandemic of our day has exacted a different sort of toll.
There looms over the world today a specter of death. Not merely the sad departure of individuals, but the loss of a greatness throughout the world that was the gathered fruit of centuries. Freedom, civic rights, the superior worth of individuals over the state, the unfettered exchange of ideas, belief in and practice of the scientific method, intellectual integrity, objective journalism, responsible government; all these former pillars of liberal society have fallen victim to the pandemic, abandoned by a populace whipped into a fearful frenzy. Something was whispered into the collective world soul in March 2020 and it now appears that it can never be unwhispered. This is a threat like nothing seen or imagined before. Everything previously held dear is up for grabs. It’s the price of survival.
And so the virus wreaks its havoc on the whole of human society in the same way that it does in the individual human body. The collected wealth and greatness of all the nations is attacked and decimated in a planet-wide cytokine storm. A new morality has come, summed up in one prime directive: Fight the virus. Good and evil are now measured against this singular objective. The destruction of wealth and freedom has been uncritically accepted for the sake of this fight—embraced and defended as necessary, while the actual effects to this day remain largely unexamined. And now the ratchet turns, and the next collateral impact is revealed: the loss of self-determination over our own bodies by decree of unelected functionaries of the state.
As the dystopian germ continues to spread through minds and institutions, those who still remember and dare to love the old way of living in the world stand and watch with mouths agape. A thing we knew yesterday only as a pathology of history now appears as a current story in our newspapers and social media feeds, and it permeates even our venerated institutions of higher learning. College and university students are being forced to receive investigational COVID vaccines that provide them little to no benefit, under pain of being denied enrollment. College administrators flatly mandate the vaccines, trading on the reduced agency of their students, who rightly fear catastrophic harm to their futures if they do not comply.
Some argue that the vaccines are not being forced on them because the students can choose not to enroll. This is a specious argument, as students understandably see a forced transfer to another school as a catastrophic disruption of their carefully laid career plans. Their choice is greatly reduced as well, since the colleges have colluded to a great extent and levied the vaccine mandates in concert. Whatever the administrators may choose to believe about alternative choices, coercion is best perceived by the one on the receiving end of it. It’s a simple fact with a thousand proofs that students are deciding to get vaccinated against their desires because the college holds all the cards. In a tragic irony of human contrivance, those least vulnerable to COVID disease are most vulnerable to vaccine coercion.
Something New Under the Sun
Some argue that vaccine mandates are nothing new, so there are no proper grounds for complaints about requiring the COVID vaccines. In fact, vaccine mandates have been increasingly abused by a corrupt system and are worthy of re-evaluation. But let us set aside that observation for our purposes here, and take care that we’re not fooled by the blatant equivocation of this argument. The differences between COVID vaccines and other vaccines are manifold. Likewise, it is one thing to vaccinate a child against a disease that is harmful to children and quite another to vaccinate a child or young adult against a disease that is almost exclusively dangerous to older adults.
The COVID vaccines are novel in several important respects: a new approach, new platforms, newly developed, and still in the beginning stages of testing. The vaccines heretofore required for children and college students are either made from attenuated/inactivated viruses or protein antigens produced under controlled conditions and designed to prime the immune system against the target pathogen. The COVID vaccines are genetic vaccines, which means that they deliver genetic material that instructs the body’s cells to produce the desired protein antigens. The difference is not trivial.1 Furthermore, the antigen produced by these genetic vaccines and protein vaccines currently in the approval pipeline is a modified SARS-CoV-2 Spike Protein. This protein has been increasingly recognized as a toxic component, possibly responsible for some or all of the more troubling outcomes in COVID patients.2 3 And growing evidence suggests that the vaccine-produced spike protein is the cause of many of the vaccine adverse side effects.
A tremendous amount of research and development effort was expended in bringing these vaccines to market, and the developers were not unaware of the issues enumerated above, as well as many more. The point here is simply that the nature of these vaccine programs is such that a rigorous and complete testing regimen is especially needed. Whether the testing was rigorous enough is a matter for debate,4 but the fact that it’s far from complete is an objective fact. The other mandated vaccines that are used to justify COVID vaccine mandates have years of safety data. We simply cannot detect a five-year or ten-year problem with 10 months of data.5 6 Some argue that if there were going to be problems, we would have seen signs of them by now. If this is so, why then do we collect long-term safety data for vaccines and use it to inform the FDA approval decision? More significantly, there are safety signals in the COVID vaccine data, and they are being left uninvestigated in some cases and explained away with deceptive analyses in others.7
In addition to the safety concerns already uncovered, there are known risks that potentially require years to manifest and can be triggered by unpredictable future events, such as the appearance of a currently unknown viral variant.8 To make matters worse, the FDA is not following their own advertised protocol for monitoring the safety of the COVID vaccines for which they provided emergency use authorization.9
Unable to Decide
So the COVID vaccines have known risks, the quantification of which is coming into focus but still developing, and potential risks that cannot now be quantified or specifically characterized. How then can one decide whether to take one of these vaccines? That’s just it; one decides. However, due to the highly stratified risk profile of COVID-19, individual deliberations on this question will vary widely. There are some people who assess that they have a high enough risk of a severe or fatal outcome from COVID that choosing to accept the risks of the vaccine instead is an easy choice. There are others in a mid-range risk stratum for whom the decision is not so easy, and they wrestle with it. And then there are the young healthy college students. There is no argument short of torturing the data that comes close to recommending, much less mandating, a blanket vaccination of college students. People in all three categories enumerated above should be left free to make their own decision about the COVID vaccines, because in all cases there is a genuine risk from the vaccine, and the person who bears in their body the consequences of the decision should be the one to make it.
Not only do college students have a vanishingly small benefit from the vaccine, which makes it less reasonable for them to assume its risks, but the risks of the vaccines are age-stratified as well—in the direction opposite to how the COVID risk stratification runs. Myocarditis and pericarditis have been identified as vaccine risk factors that vary inversely with age, and there is emerging evidence to suggest that the same may be true with respect to the serious CNS disease Guillain-Barre Syndrome.10 The CDC’s handling of the reports of vaccine-induced myocarditis and pericarditis in children is emblematic of the prioritization of vaccine uptake numbers over safety, culminating in an advisory committee meeting that was downright scandalous in its handling of safety concerns for children.11
Additionally, college students have more remaining life expectancy being put at risk than mature adults have. The risk of developing MS or ALS or a permanent autoimmune disease 20 years after injection of the vaccine may not be a serious concern to a 70-year-old. But a 20-year-old has a great deal more reason to be concerned about this risk. To force him or her to receive the vaccine in the face of this risk is nothing short of unconscionable.
All Risk No Benefit
Safety concerns with the COVID vaccines represent only one side of a two-factor trade-off. The risk of harm is to be balanced against the expected benefit. This is a bedrock principle of modern medicine, but it is being scandalously flouted by doctors and public health authorities in blind pursuit of the prime directive to fight the virus. Healthy college students have a statistically zero risk of dying from COVID, but there is a small, yet discernible, risk for them of being killed by the vaccine. More significantly, there is an unquantified risk of significant harm from the vaccine. Not a purely speculative “something might go wrong” risk, but known failure modes of these particular vaccines which require more time to manifest than has so far elapsed since the development of the new vaccine platforms.
To take only one example, consider how we might answer this important question: Given the results of in-vitro and animal model studies which indicate spike protein trafficking in large quantities to the ovaries and other reproductive organs,12 what is the risk that 18-year-old to 24-year-old students who take the vaccines now as required by the mandates receive significant harm to their reproductive abilities? We can only answer that question now with a time machine. The magnitude of the risk will be unknown until we travel naturally into that future. Taking a risk that is unquantifiable as the cost of mitigating a better-known risk can be a reasonable course of action. Assuming such a risk for no discernible benefit is foolhardy. Forcing someone to assume such a risk for no discernible benefit is morally repugnant and an assault on their bodily integrity and personal freedom.
But can such a thing be required for the good of society? That may very well be the underlying motivation for mandating the COVID vaccines, although the policies are typically couched in “keeping the students safe” language. This is not surprising, because there are two monumental problems with admitting that college students are being forced to take on a health risk for which others, not the vaccinated student, bear the benefit. Firstly, no one in a free and moral society has the right to force such a decision on someone else. Secondly, if we drop from our minds and hearts the March 2020 view of COVID and make a clear-eyed assessment of what we know now, it becomes clear that there is no crisis to justify the extraordinary step of assuming control over college students’ bodily health, and that universal vaccination is far from being the best, much less the only, means of restoring normalcy to college campuses.
For a number of reasons, COVID mortality is now understood to be far less than originally thought.13 Previously censored information has now removed all doubt that there are safe, cheap, and effective preventive measures and treatments for COVID. Vaccines are far from the only effective option for responding to the threat of COVID.14 There are indications that vaccines, while protecting against moderate or serious COVID disease, are not so effective at reducing the spread of the virus. The risk of pathogenic priming and vaccine-enhanced disease will always be a possibility with the COVID vaccines.15 Natural immunity is superior to vaccine-induced immunity, despite the Orwellian attempt by vaccine supporters to remove it from consideration.
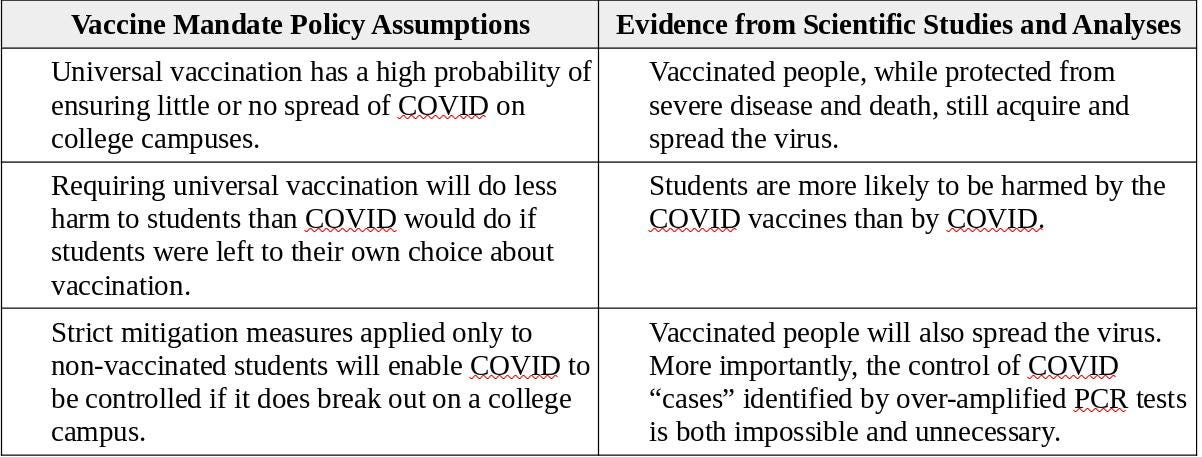
Every one of the foregoing observations undercuts the rationale for the COVID vaccine mandates, which presuppose the accuracy of a narrow set of assertions that are pointedly challenged by a wide variety of credentialed experts in various scientific, medical, and public health disciplines. This discrepancy is illustrated in the following table.
In mandating the vaccines, colleges and universities are not merely taking the wrong side in the debate. They’re unable or unwilling to engage in the discussion, trusting blindly in agenda-driven pronouncements by health agencies that ignore what every attentive reader knows has been reliably established by scientific analyses unfettered by a-priori policy commitments.
No just and moral society can permit the well-being of young adults and children to be sacrificed for the benefit of their elders. Yet this assault on our university and college students is merely the first rustling of an ill wind. The relentless drive to give the COVID vaccines to younger and younger children warns of a catastrophic sequel, with mandates for the children likely to follow if we fail to oppose what is being done to adolescents and young adults.
The Delta Effect
With the Fall semester rapidly approaching, the Delta variant is being hyped as a reason to re-instate COVID mitigation measures only recently rescinded and to double down on vaccination efforts, including mandates for college and university students. By emphasizing cases over hospitalizations and deaths, health authorities and media pandemic promoters are obscuring the fact that the Delta variant is a welcome development, a less virulent virus spreading more readily than more dangerous strains, possibly signaling the end of the pandemic.16 Furthermore, data from Israel and the UK indicate that the Delta variant is infecting vaccinated and non-vaccinated people in equal proportions.17 This observation will likely hold in every country where the Delta variant becomes the dominant strain, reducing the benefit of the vaccine, especially for young people who are at zero statistical risk of death even from the more virulent COVID strains.
A Certain Future and a Changing Past
Despite how it may seem now, this long dystopian chapter in our history will end. Those who come after us will have the luxury of assessing these events with patient, penetrating reason rather than fear. We would all do well to adopt that posture now. Yet even before these events are subsumed into a set of historical data to be dispassionately mined and analyzed, they will be subject to the reckoning that is even now coming into focus. Comparisons among states and countries with widely varying anti-COVID measures already provide evidence of the uselessness, and even harmfulness, of measures taken ostensibly for the public good.
A similar divide among colleges and universities will tell its tale before long. And that tale will have increasing significance as the long-term safety of the vaccines is no longer merely the subject of analytic models and crafty explanations, but is evident in the actual health outcomes of those forced to take the vaccines. Institutions making policy decisions now in the midst of these times that are trying the nation’s soul will all stand before the bar of history. Those who usurped the freedom of their students in pursuit of the fear-driven prime directive to fight the virus, and those who maintained their trust in individuals to act well in their own interests, will all be assessed in the cool light of historical analysis. Institutions of higher learning must decide now in which group they will stand.
The genetic material requires a specialized delivery system—DNA spliced into a genetically engineered Adenovirus or mRNA wrapped in a Lipid Nano Particle (LNP). These are high-tech, complex systems that have been in development for years. Several thorny issues required resolution, pertaining to the genetic code itself (https://tinyurl.com/ab86z7me) as well as the delivery mechanism (https://tinyurl.com/4hh3fck7). The mediation of antigen production by the body’s genetic machinery is a factor not present with traditional vaccines. See Notes 2 and 3 for a discussion of toxic effects of the spike protein antigen, Note3 4 and 12 for significant open questions about the bio-distribution of the LNP wrappers, and Notes 5 and 6 for a discussion of long-term vaccine effects on immune system functioning.
An in-vitro study demonstrated that the Spike Protein compromises the blood-brain barrier. (https://tinyurl.com/y9pa247d).
An animal study found immune system activation in brain cells and the formation of Lewy bodies (a marker for Parkinson's disease) apparently induced by the S1 subunit of the Spike Protein (https://tinyurl.com/yv42atp8).
The regulators agreed to skip human bio-distribution studies, which is a curious decision when complex novel platforms were being developed and plans were underway to vaccinate nearly every person on the planet. (See this BMJ article: https://tinyurl.com/7mt7dy5b). If animal safety studies were done, they’re not readily available. It’s also important to note that the vaccine manufacturers destroyed the placebo arm of the trial after the EUA was granted. So we have a 3-month RCT that has ended, and an ongoing observational study with no control.
See extended discussion among several scientists and doctors, initiated by Dr. JW Ulm, in the comments section of this article: https://tinyurl.com/4hh3fck7. There is general consensus that the long-term safety of the vaccines cannot be assumed from the available trial data, apart from technical information on the LNP wrapper composition that the vaccine manufacturers have declined to disclose. Specific scenarios are discussed in which MS, ALS, chronic autoimmune disease, and other pathologies could subsist in a subclinical form and manifest years or decades after injection, as bio-distribution, tissue affinity, and other effects are highly dependent on the details of LNP composition. These issues were prominent challenges throughout the 10+ years of mRNA technology development. Thus it’s highly unlikely that specific studies were not done, and the failure of vaccine manufacturers to provide relevant information is troubling.
The probability of long-term manifestation of CNS, autoimmune, and other diseases increases with repeated vaccine dosing. Many experts warning of possible widespread injury from the COVID vaccines have said that the implementation of a regular booster shot regimen is where the risk of catastrophic damage lies.
See, for example, this WSJ article (https://tinyurl.com/v4r4dx6m) written by a Johns Hopkins School of Medicine professor. He demonstrates numerous problems with CDC’s analysis purporting to show greater risk to children from COVID than from the vaccine. This is one of many doctors and scientists making such observations. These are troubling indications that CDC worked backward from the answer to the analysis to the data, to assert that vaccines are safe and effective.
Antibody-Dependent Enhancement (ADE) is a known vaccine risk that is especially relevant to coronavirus vaccines. It can have catastrophic effects on a population when it occurs. This article (https://tinyurl.com/59phmz75) describes the two main ADE mechanisms and concludes that “Given past data on multiple SARS-CoV-1 and MERS-CoV vaccine efforts have failed due to ADE in animal models (75, 81), it is reasonable to hypothesize a similar ADE risk for SARS-CoV-2 antibodies and vaccines.” Several months into the vaccination program, evidence has emerged that mutations presented in the Delta variant make the prospect of ADE more likely than was originally claimed. See https://www.biorxiv.org/content/10.1101/2021.08.22.457114v1
“Please see this set of slides Oct 22, 2020, FDA VRBAC meeting indicating the vast array of data systems that were going to be used to track safety issues with the COVID-19 vaccines and give the public and doctors real-time information to make decisions or for the CDC/FDA to perform risk mitigation. To this day there has not been a single press briefing on overall safety nor any mention of data beyond VAERS and V-safe and no hint of risk mitigation.” -Dr. Peter McCullough, referring to the FDA safety protocol documented here: https://tinyurl.com/a5rvunnu
See https://tinyurl.com/4ptbrnbk (full article behind a paywall)
The Advisory Committee for Immunization Practices (ACIP), a CDC committee that makes recommendations on how to use vaccines to control diseases in the U.S, called an emergency meeting for June 18 to deal with an emerging safety signal in the vaccine data concerning myocarditis and pericarditis in teens and young adults. After announcing a one-week delay on the eve of the emergency meeting because it fell on the Juneteenth holiday, the committee recommended one week later that vaccinations should continue for young people because “the benefits continue to outweigh the risks.” This was based on their assessment that most cases of myocarditis were mild, and teens were only briefly hospitalized. Myocarditis is evidence of cardiac damage. Many of these teens will be told they cannot exercise or engage in sports for extended periods of time, many must remain on cardiac medications, and they face an increased risk of heart failure in the future. Furthermore, the myocarditis risk for young people was understated by using dilated age bands that enabled older subjects to dilute the prevalence numbers for younger subjects, given that the prevalence increases sharply with decreasing age. Likewise, the COVID risk for young children was overstated by Using COVID hospitalization rates for young people that CDC themselves determined were near twice the actual rate of COVID-induced hospitalization, because they included kids hospitalized for unrelated causes who happened to test positive for COVID. Finally, the risk/benefit calculation was skewed by confounding healthy and sick people in the comparison. Children and college-aged kids hospitalized for COVID are almost all suffering from serious comorbidities, while the vaccines are being pushed on healthy teens and college students.
See this animal model bio-distribution study: https://tinyurl.com/yf49nec5. See also the BMJ article in Note 4 pointing out the unfortunate decision to skip human bio-distribution studies for the COVID vaccines.
A range of Infection Fatality Rate (IFR) estimates may be found, since it depends on an estimate of the seroprevalence of the virus. In general, however, the IFR is taken to be at least an order of magnitude lower than the consensus value in the Spring of 2020, when public perceptions and mitigation strategies that persist today were first formed.
See the following protocols developed by several coalitions of doctors who are collectively treating thousands of COVID-19 patients: https://aapsonline.org/CovidPatientTreatmentGuide.pdf , https://covid19criticalcare.com/covid-19-protocols, / https://swprs.org/on-the-treatment-of-covid-19/
See Note 8.
https://tinyurl.com/vn3yw8x6. This observation made in August appears now (Jan 2022) to be incorrect. Delta seems to have become more dangerous throughout the Summer of 2021, with the CFR rising in apparent correlation with vaccine rollout. This may have been driven by the reverse evolutionary pressure applied by attempted universal vaccination with a leaky vaccine during a pandemic (see https://boriquagato.substack.com/p/are-leaky-vaccines-driving-delta). At any rate, Omicron is here now, and it is widely recognized to be significantly less dangerous than Delta and other previous strains. It shifts the risk-benefit tradeoff for the vaccines in the direction of risk, perhaps an order of magnitude more than Delta appeared to do so in August 2021.
Hi Mark,
Thank you so much for putting this information together; it is incredibly helpful. Do you know the exemption specifics of particular colleges, by college? Do you know of an online site where parents can figure out if a college allows for religious or medical exemptions?